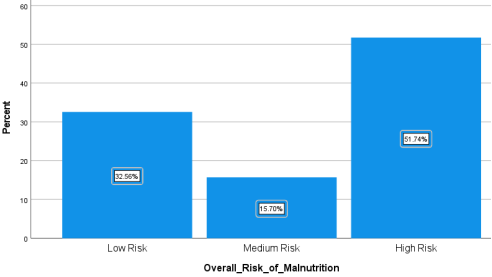
The global attainment of the Sustainable Development Goal 3 target 3.4 has been slow, with a notable increase in the cancer burden. Besides the normal cancer pathogenesis, 5-10% of the total cancer cases develop as a result of sub-optimal diets and other lifestyle factors and therefore, consuming a healthy diet in adequate amounts helps in prevention of the tumor itself and cancer related malnutrition. Limited evidence exists on the link between dietary practices and the nutrition status of cancer patients, and this study sought to fill this gap using analytical cross-sectional study design. Data was collected using a 24-hour recall, Food Frequency Questionnaire and Malnutrition Universal Screening Tool. The dietary patterns identified from the research were, excessive consumption of foods from the starchy foods and the fats category (65.1%) with less than half (41.9%) of the respondents not attaining the minimum daily requirements of the fruit’s servings recommended by World Health Organization (WHO). The mean energy intake of the 172 respondents was below the ESPEN Clinical guidelines recommendations. More than half (51.7%) of the respondents were at a high risk of developing malnutrition and there was a statistically significant difference between individual energy intake and the nutrition status (P<0.05) rejecting the null hypothesis that there is no significant association between the energy intake and the risk of being malnourished. Linear regression r (0.41) showed a significant (P<0.05) weak positive association between a person’s diet intake and the malnutrition risk. The analysis shows that 16.7% of the overall risk of malnutrition can be explained by the dietary intake. Assessing the dietary practices of the cancer patients, screening them for malnutrition risk and enhancing nutrition education and counselling is key in improving therapeutic care of cancer patients. A study to reveal the knowledge and attitudes of the cancer patients towards these dietary practices would make a very significant contribution to the therapeutic care of the cancer patients.
| Published in | International Journal of Nutrition and Food Sciences (Volume 13, Issue 6) |
| DOI | 10.11648/j.ijnfs.20241306.11 |
| Page(s) | 239-248 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Dietary Practices, Malnutrition Universal Screening Tool, Nutrition Status, Malnutrition Risk, 24-hour Recall
Respondent’s Characteristics | Frequency | Percent (%) |
|---|---|---|
Respondents gender | N=172 | |
Male | 67 | 39.0 |
Female | 105 | 61.0 |
Religion | ||
Christianity | 165 | 95.9 |
Muslim | 7 | 4.1 |
Respondent’s education level | ||
Primary | 105 | 61.0 |
Secondary | 50 | 29.1 |
College | 16 | 9.3 |
University | 1 | .60 |
Marital Status of the respondents | ||
Married | 125 | 72.7 |
Single | 31 | 18.0 |
Widowed/Deceased | 16 | 9.3 |
Monthly Income | ||
0-10,000 | 86 | 50.0 |
10,000-20,000 | 49 | 28.5 |
20,000-50,000 | 32 | 18.6 |
50,000-100,000 | 5 | 2.9 |
Minimum | Maximum | Mean | S. D | |
|---|---|---|---|---|
Energy | 169.30 | 3283.30 | 1068.61 | 520.62639 |
Water | 240.80 | 3288.00 | 959.365 | 361.86533 |
Protein | 5.50 | 443.40 | 46.8308 | 42.66351 |
Fat | .00 | 154.80 | 27.1380 | 27.57125 |
Carbohydrate | 2.20 | 434.50 | 112.922 | 83.49550 |
Dietary Fiber | 3.10 | 68.40 | 20.6814 | 12.21267 |
Alcohol | .00 | 272.10 | 46.1819 | 77.37332 |
PFA | .00 | 102.00 | 9.8035 | 14.78217 |
Cholesterol | .00 | 1102.70 | 92.2727 | 210.72963 |
Vitamin A | .00 | 23858.30 | 1137.71 | 2846.01160 |
Carotene | .00 | 7595.60 | 595.959 | 1310.93351 |
Vitamin E | .00 | 643.50 | 32.0442 | 101.53486 |
Vitamin B1 | .10 | 2942.00 | 278.205 | 646.14196 |
Vitamin B2 | .00 | 5892.70 | 107.107 | 618.01408 |
Vitamin B6 | .00 | 3.00 | .5390 | .64513 |
Folic Acid | .00 | 1213.80 | 187.581 | 239.61854 |
Vitamin C | .10 | 436.30 | 78.6814 | 79.17806 |
Sodium | .70 | 5551.00 | 911.995 | 1087.75025 |
Potassium | 165.30 | 8290.50 | 2105.25 | 1083.95038 |
Calcium | 28.00 | 1704.50 | 416.126 | 269.89709 |
Magnesium | 32.00 | 623.70 | 224.268 | 95.84983 |
Phosphorus | 98.00 | 3276.00 | 849.868 | 423.89742 |
Iron | 1.20 | 41.50 | 10.6581 | 6.20451 |
Zinc | .90 | 28.30 | 6.2738 | 4.58614 |
% FREQUENCY (N=172) | ||||
|---|---|---|---|---|
Food Group | Daily | Weekly | Rarely | Average Serving |
Starchy foods | 65.1 | 34.9 | 0 | Large (65.1%) |
Vegetables | 57.6 | 42.4 | 0 | Large (48.8%) |
Fruits | 41.9 | 55.8 | 2.3 | Small (40.7%) |
Legumes and pulses | 60.5 | 37.8 | 1.7 | Large (55.2%) |
Nuts and seeds | 8.7 | 44.2 | 47.1 | Small (73.3%) |
Meat, fish, animal protein | 15.1 | 74.4 | 10.5 | Small (61.1%) |
Milk and milk products | 37.8 | 43.0 | 19.2 | Small (47.1%) |
Fats and oils | 65.1 | 27.9 | 7.0 | Large (55.8%) |
Sugar and sweets | 33.1 | 33.7 | 33.1 | Small (47.1%) |
Condiments, spices and beverages | 8.1 | 19.2 | 72.7 | Small (83.7%) |
Alcohol | 2.3 | 2.9 | 94.8 | Small (95.3%) |
R Square | B | Std. Error | Beta | Significance | |
|---|---|---|---|---|---|
.408a | .167 | 1.388 | .157 | .000 | |
.000 | .000 | -.106 | .167 |
ESPEN | European Society for Clinical Nutrition and Metabolism |
FFQ | Food Frequency Questionnaire |
MUST | Malnutrition Universal Screening Tool |
BMI | Body Mass Index |
NCRH | Nyeri County Referral Hospital |
| [1] | Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer JClin2021; 71: 209–49. |
| [2] | Morze J, Danielewicz A, Przybyłowicz K, Zeng H, Hoffmann G, Schwingshackl L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur J Nutr 2021; 60: 1561–86. |
| [3] | Muscaritoli M, Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin Nutr 2021; 40: 2898–913. |
| [4] | Wang Y, Liu K, Long T, Long J, Li Y, Li J, et al. Dietary fish and omega-3 polyunsaturated fatty acids intake and cancer survival: A systematic review and meta-analysis. Crit Rev Food Sci Nutr 2023; 63: 6235–51. |
| [5] | Naghshi S, Sadeghi O, Willett WC, Esmaillzadeh A. Dietary intake of total, animal, and plant proteins and risk of all cause, cardiovascular, and cancer mortality: Systematic review and dose-response meta-analysis of prospective cohort studies. The BMJ 2020; 370. |
| [6] | Ministry of Health Kenya. National Guidelines for Healthy Diets. Natl Guidel Healthy Diets Phys Act 2017. |
| [7] | American Cancer Society. Nutrition for People with Cancer Benefits of good nutrition during cancer treatment 2018: 1–27. |
| [8] | Bhosale PB, Ha SE, Vetrivel P, Kim HH, Kim SM, Kim GS. Functions of polyphenols and its anticancer properties in biomedical research: A narrative review. Transl Cancer Res 2020; 9: 7619–31. |
| [9] | Radomska D, Czarnomysy R, Radomski D, Bielawska A, Bielawski K. Selenium as a bioactive micronutrient in the human diet and its cancer chemopreventive activity. Nutrients 2021; 13: 1–25. |
| [10] | Opanga Y, Kaduka L, Bukania Z, Mutisya R, Korir A, Thuita V, et al. Nutritional status of cancer outpatients using scored patient generated subjective global assessment in two cancer treatment centers, Nairobi, Kenya. BMC Nutr 2017; 3: 1–7. |
| [11] | Sissung TM, Cordes LM, Figg WD. Perspectives Quackery the Dietary Supplement Health and Education Act: are we healthier and better informed after 27 years? Lancet Oncol 2021; 22: 915–6. |
| [12] | Muscaritoli M, Lucia S, Farcomeni A, Lorusso V, Saracino V, Barone C, et al. Prevalence of malnutrition in patients at first medical oncology visit: The PreMiO study. Oncotarget 2017; 8: 79884–96. |
| [13] | Choi JY, Lee JH, Song YJ. Evaluation of Iodine Status among Korean Patients with Papillary Thyroid Cancer Using Dietary and Urinary Iodine. Endocrinol Metab 2021; 36: 607–18. |
| [14] | Gomes-Neto AW, Vliet IMY van, Osté MCJ, Jong MFC de, Bakker SJL, Jager-Wittenaar H, et al. Malnutrition Universal Screening Tool and Patient-Generated Subjective Global Assessment Short Form and their predictive validity in hospitalized patients. Clin Nutr ESPEN 2021; 45: 252–61. |
| [15] | Wambalaba FW, Son B, Wambalaba AE, Nyong’o D, Nyong’o A. Prevalence and Capacity of Cancer Diagnostics and Treatment: A Demand and Supply Survey of Health-Care Facilities in Kenya. Cancer Control 2019; 26: 1–12. |
| [16] | NCIDP 2013-2017. Republic of Kenya Nyeri County Intergrated Development Plan 2013-2017 Department of Finance and Economic Planning 2013: 324. |
| [17] | Sun Y, Phillips PCB. Understanding the Fisher equation. J Appl Econom 2004; 19: 869–86. |
| [18] | Auma CMN, Mweu MM, Opiyo RO. Performance of Malnutrition Universal Screening Tool and Patient-Generated Global Subjective Assessment in screening for cancer-related malnutrition in Nairobi, Kenya. F1000Research 2022; 11: 755. |
| [19] | Danner D. Reliability – The Precision of a Measurement. GESIS Surv Guidel 2016. |
| [20] | Laky B, Janda M, Kondalsamy-Chennakesavan S, Cleghorn G, Obermair A. Pretreatment malnutrition and quality of life - association with prolonged length of hospital stay among patients with gynecological cancer: A cohort study. BMC Cancer 2010; 10. |
| [21] | Bradbury KE, Murphy N, Key TJ. Diet and colorectal cancer in UK Biobank: A prospective study. Int J Epidemiol 2020; 49: 246–58. |
| [22] | Thompson FE, Subar AF. Dietary Assessment Methodology. 2017. |
| [23] | Fincham JE. Response rates and responsiveness for surveys, standards, and the Journal. Am J Pharm Educ 2008; 72: 43. |
| [24] | Hinata A, Kabasawa K, Watanabe Y, Kitamura K, Ito Y, Takachi R, et al. Education, household income, and depressive symptoms in middle-aged and older Japanese adults. BMC Public Health 2021; 21: 1–10. |
| [25] | Krajc K, Miroševič Š, Sajovic J, Klemenc Ketiš Z, Spiegel D, Drevenšek G, et al. Marital status and survival in cancer patients: A systematic review and meta‐analysis. Cancer Med 2023; 12: 1685–708. |
| [26] | Rock CL, Thomson C, Gansler T, Gapstur SM, Mccullough ML, Patel AV, et al. American Cancer Society Guideline for Diet and Physical Activity for Cancer Prevention 2020; 70: 245–71. |
| [27] | de Pinho NB, Martucci RB, Rodrigues VD, D’Almeida CA, Thuler LCS, Saunders C, et al. Malnutrition associated with nutrition impact symptoms and localization of the disease: Results of a multicentric research on oncological nutrition. Clin Nutr 2019; 38: 1274–9. |
| [28] | Lega IC, Lipscombe LL. Review: Diabetes, Obesity, and Cancer-Pathophysiology and Clinical Implications. Endocr Rev 2020; 41: 33–52. |
| [29] | Nagy S, Petrosky SN, Beckler MD, Kesselman MM. The Impact of Modern Dietary Practices on Cancer Risk and Progression: A Systematic Review. Cureus 2023. |
| [30] | Hanson S, Thorpe G, Winstanley L, Abdelhamid AS, Hooper L, Abdelhamid A, et al. Omega-3, omega-6 and total dietary polyunsaturated fat on cancer incidence: systematic review and meta-analysis of randomised trials. Br J Cancer 2020; 122: 1260–70. |
| [31] | Anderson NM, Simon MC. The tumor microenvironment. Curr Biol 2020; 30: R921–5. |
| [32] | Oduor EA, Odongo AO, Kiboi W. Dietary Practices and Nutritional Status of Adult Cancer Patients: A Case Study of Texas Cancer Center, Kenya. Int J Trop Dis Health 2024; 45: 36–44. |
APA Style
Bundi, D., Chege, P., Kamuhu, R. (2024). Association Between the Dietary Practices and the Nutrition Status of Adult Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey. International Journal of Nutrition and Food Sciences, 13(6), 239-248. https://doi.org/10.11648/j.ijnfs.20241306.11
ACS Style
Bundi, D.; Chege, P.; Kamuhu, R. Association Between the Dietary Practices and the Nutrition Status of Adult Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey. Int. J. Nutr. Food Sci. 2024, 13(6), 239-248. doi: 10.11648/j.ijnfs.20241306.11
AMA Style
Bundi D, Chege P, Kamuhu R. Association Between the Dietary Practices and the Nutrition Status of Adult Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey. Int J Nutr Food Sci. 2024;13(6):239-248. doi: 10.11648/j.ijnfs.20241306.11
@article{10.11648/j.ijnfs.20241306.11,
author = {Dorothy Bundi and Peter Chege and Regina Kamuhu},
title = {Association Between the Dietary Practices and the Nutrition Status of Adult Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey
},
journal = {International Journal of Nutrition and Food Sciences},
volume = {13},
number = {6},
pages = {239-248},
doi = {10.11648/j.ijnfs.20241306.11},
url = {https://doi.org/10.11648/j.ijnfs.20241306.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijnfs.20241306.11},
abstract = {The global attainment of the Sustainable Development Goal 3 target 3.4 has been slow, with a notable increase in the cancer burden. Besides the normal cancer pathogenesis, 5-10% of the total cancer cases develop as a result of sub-optimal diets and other lifestyle factors and therefore, consuming a healthy diet in adequate amounts helps in prevention of the tumor itself and cancer related malnutrition. Limited evidence exists on the link between dietary practices and the nutrition status of cancer patients, and this study sought to fill this gap using analytical cross-sectional study design. Data was collected using a 24-hour recall, Food Frequency Questionnaire and Malnutrition Universal Screening Tool. The dietary patterns identified from the research were, excessive consumption of foods from the starchy foods and the fats category (65.1%) with less than half (41.9%) of the respondents not attaining the minimum daily requirements of the fruit’s servings recommended by World Health Organization (WHO). The mean energy intake of the 172 respondents was below the ESPEN Clinical guidelines recommendations. More than half (51.7%) of the respondents were at a high risk of developing malnutrition and there was a statistically significant difference between individual energy intake and the nutrition status (P<0.05) rejecting the null hypothesis that there is no significant association between the energy intake and the risk of being malnourished. Linear regression r (0.41) showed a significant (P<0.05) weak positive association between a person’s diet intake and the malnutrition risk. The analysis shows that 16.7% of the overall risk of malnutrition can be explained by the dietary intake. Assessing the dietary practices of the cancer patients, screening them for malnutrition risk and enhancing nutrition education and counselling is key in improving therapeutic care of cancer patients. A study to reveal the knowledge and attitudes of the cancer patients towards these dietary practices would make a very significant contribution to the therapeutic care of the cancer patients.
},
year = {2024}
}
TY - JOUR T1 - Association Between the Dietary Practices and the Nutrition Status of Adult Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey AU - Dorothy Bundi AU - Peter Chege AU - Regina Kamuhu Y1 - 2024/11/18 PY - 2024 N1 - https://doi.org/10.11648/j.ijnfs.20241306.11 DO - 10.11648/j.ijnfs.20241306.11 T2 - International Journal of Nutrition and Food Sciences JF - International Journal of Nutrition and Food Sciences JO - International Journal of Nutrition and Food Sciences SP - 239 EP - 248 PB - Science Publishing Group SN - 2327-2716 UR - https://doi.org/10.11648/j.ijnfs.20241306.11 AB - The global attainment of the Sustainable Development Goal 3 target 3.4 has been slow, with a notable increase in the cancer burden. Besides the normal cancer pathogenesis, 5-10% of the total cancer cases develop as a result of sub-optimal diets and other lifestyle factors and therefore, consuming a healthy diet in adequate amounts helps in prevention of the tumor itself and cancer related malnutrition. Limited evidence exists on the link between dietary practices and the nutrition status of cancer patients, and this study sought to fill this gap using analytical cross-sectional study design. Data was collected using a 24-hour recall, Food Frequency Questionnaire and Malnutrition Universal Screening Tool. The dietary patterns identified from the research were, excessive consumption of foods from the starchy foods and the fats category (65.1%) with less than half (41.9%) of the respondents not attaining the minimum daily requirements of the fruit’s servings recommended by World Health Organization (WHO). The mean energy intake of the 172 respondents was below the ESPEN Clinical guidelines recommendations. More than half (51.7%) of the respondents were at a high risk of developing malnutrition and there was a statistically significant difference between individual energy intake and the nutrition status (P<0.05) rejecting the null hypothesis that there is no significant association between the energy intake and the risk of being malnourished. Linear regression r (0.41) showed a significant (P<0.05) weak positive association between a person’s diet intake and the malnutrition risk. The analysis shows that 16.7% of the overall risk of malnutrition can be explained by the dietary intake. Assessing the dietary practices of the cancer patients, screening them for malnutrition risk and enhancing nutrition education and counselling is key in improving therapeutic care of cancer patients. A study to reveal the knowledge and attitudes of the cancer patients towards these dietary practices would make a very significant contribution to the therapeutic care of the cancer patients. VL - 13 IS - 6 ER -
Institute of Food Bioresources Technology, Dedan Kimathi University of Technology, Nyeri, Kenya
Biography: Dorothy Kareainto Bundi is a Nutrition technologist at Dedan Kimathi University of Technology. She is a master’s student at Kenyatta University and holds a Bachelor’s degree from Egerton University, (2015).
Research Fields: Non-communicable Diseases and nutrition, Maternal and Child Nutrition.

School of Health Sciences, Kenyatta University, Nairobi, Kenya
Biography: Peter Chege is a senior lecturer at Kenyatta University. He holds a PhD and a Masters degree from Kenyatta University.
Research Fields: Agri-nutrition, Community nutrition, Food security, Micronutrients, Livelihood studies

School of Health Sciences, Kenyatta University, Nairobi, Kenya
Biography: Regina Kamuhu Is a lecturer at Kenyatta University Department of Foods, Nutrition and Dietetics. She holds a PhD in Foods, Nutrition and Dietetics from Kenyatta University- 2016 and a Master’s degree from University of Panjab, India.
Research Fields: HIV dyslipidaemia, Utilization of groundnuts/ peanut in treatment of lipid disorders in HIV and diabetes.